Free Hawaii Hc 5 Template
Free Hawaii Hc 5 Template
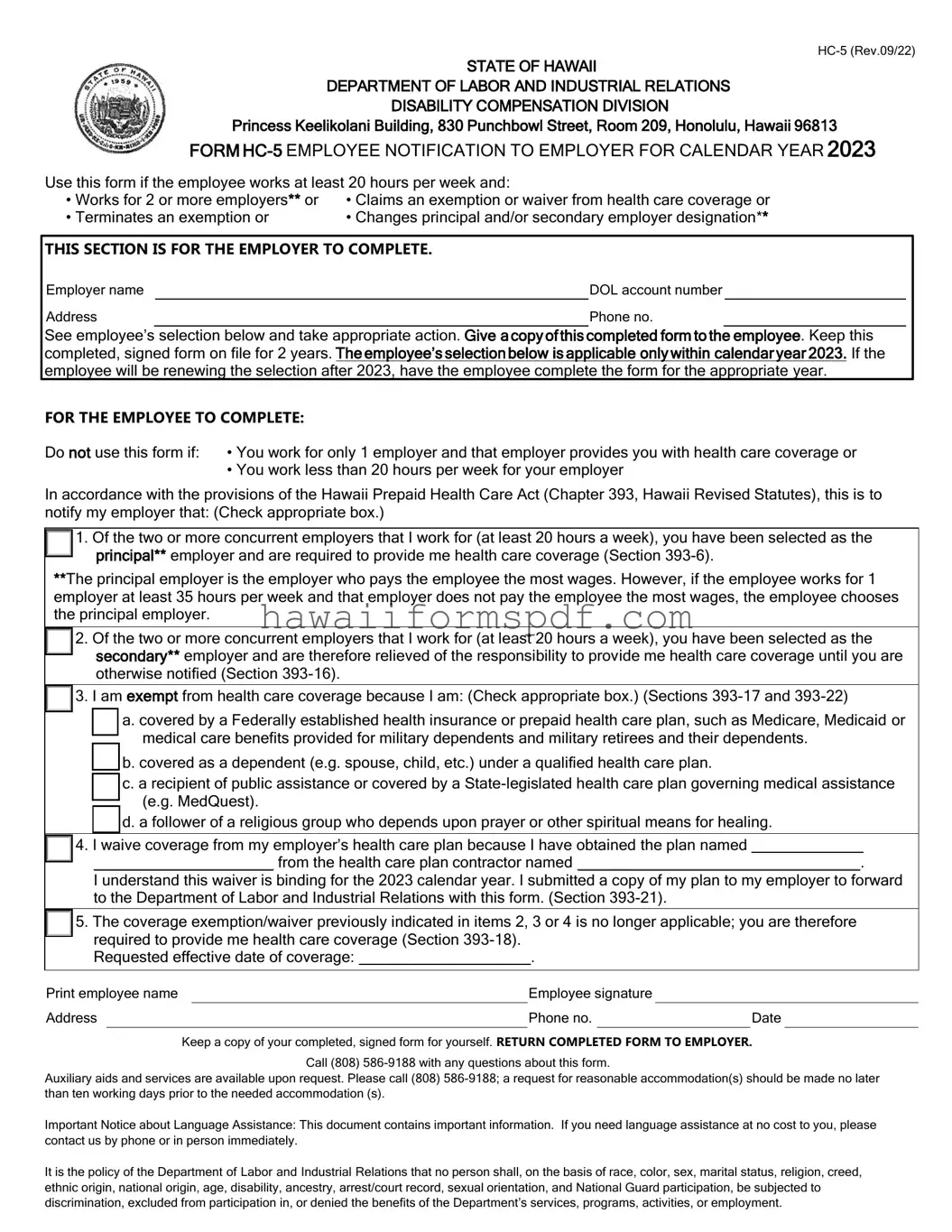
The Hawaii HC-5 form plays a vital role in ensuring that employees understand their rights and responsibilities regarding health care coverage under the Hawaii Prepaid Health Care Act. This form is specifically designed for employees who work for two or more employers or those who wish to claim an exemption or waiver from health care coverage. It allows individuals to notify their principal and secondary employers about their health care coverage status. Employees must complete the form accurately, indicating whether they have selected a principal employer responsible for providing health care coverage or a secondary employer who is relieved of this responsibility. Additionally, the form addresses various scenarios, such as exemptions due to coverage by federal health plans or other qualifying conditions. Employees should keep a signed copy for their records and submit the completed form to their employer, who is required to retain it for two years. By understanding and utilizing the HC-5 form, employees can navigate their health care coverage options more effectively, ensuring compliance with state regulations while protecting their health care rights.
STATE OF HAWAII
DEPARTMENT OF LABOR AND INDUSTRIAL RELATIONS
DISABILITY COMPENSATION DIVISION
Princess Keelikolani Building, 830 Punchbowl Street, Room 209, Honolulu, Hawaii 96813
FORM
Use this form if the employee works at least 20 hours per week and:
•Works for 2 or more employers** or • Claims an exemption or waiver from health care coverage or
• Terminates an exemption or |
• Changes principal and/or secondary employer designation** |
|
|||
|
|
||||
THIS SECTION IS FOR THE EMPLOYER TO COMPLETE. |
|
||||
Employer name |
|
|
DOL account number |
|
|
Address |
|
Phone no. |
|
||
See employee’s selection below and take appropriate action. Give a copy of this completed form to the employee. Keep this completed, signed form on file for 2 years. The employee’s selection below is applicable only within calendar year 2023. If the employee will be renewing the selection after 2023, have the employee complete the form for the appropriate year.
FOR THE EMPLOYEE TO COMPLETE:
Do not use this form if: • You work for only 1 employer and that employer provides you with health care coverage or
•You work less than 20 hours per week for your employer
In accordance with the provisions of the Hawaii Prepaid Health Care Act (Chapter 393, Hawaii Revised Statutes), this is to notify my employer that: (Check appropriate box.)

 1. Of the two or more concurrent employers that I work for (at least 20 hours a week), you have been selected as the principal** employer and are required to provide me health care coverage (Section
1. Of the two or more concurrent employers that I work for (at least 20 hours a week), you have been selected as the principal** employer and are required to provide me health care coverage (Section
**The principal employer is the employer who pays the employee the most wages. However, if the employee works for 1 employer at least 35 hours per week and that employer does not pay the employee the most wages, the employee chooses the principal employer.

 2. Of the two or more concurrent employers that I work for (at least 20 hours a week), you have been selected as the secondary** employer and are therefore relieved of the responsibility to provide me health care coverage until you are otherwise notified (Section
2. Of the two or more concurrent employers that I work for (at least 20 hours a week), you have been selected as the secondary** employer and are therefore relieved of the responsibility to provide me health care coverage until you are otherwise notified (Section

 3. I am exempt from health care coverage because I am: (Check appropriate box.) (Sections
3. I am exempt from health care coverage because I am: (Check appropriate box.) (Sections

 a. covered by a Federally established health insurance or prepaid health care plan, such as Medicare, Medicaid or medical care benefits provided for military dependents and military retirees and their dependents.
a. covered by a Federally established health insurance or prepaid health care plan, such as Medicare, Medicaid or medical care benefits provided for military dependents and military retirees and their dependents.

 b. covered as a dependent (e.g. spouse, child, etc.) under a qualified health care plan.
b. covered as a dependent (e.g. spouse, child, etc.) under a qualified health care plan.

 c. a recipient of public assistance or covered by a
c. a recipient of public assistance or covered by a

 d. a follower of a religious group who depends upon prayer or other spiritual means for healing.
d. a follower of a religious group who depends upon prayer or other spiritual means for healing.

 4. I waive coverage from my employer’s health care plan because I have obtained the plan named _____________
4. I waive coverage from my employer’s health care plan because I have obtained the plan named _____________
_____________________ from the health care plan contractor named _________________________________.
I understand this waiver is binding for the 2023 calendar year. I submitted a copy of my plan to my employer to forward to the Department of Labor and Industrial Relations with this form. (Section

 5. The coverage exemption/waiver previously indicated in items 2, 3 or 4 is no longer applicable; you are therefore required to provide me health care coverage (Section
5. The coverage exemption/waiver previously indicated in items 2, 3 or 4 is no longer applicable; you are therefore required to provide me health care coverage (Section
Requested effective date of coverage: ____________________.
Print employee name |
|
|
Employee signature |
|
|
|
||
Address |
|
|
|
Phone no. |
|
|
Date |
|
|
|
Keep a copy of your completed, signed form for yourself. RETURN COMPLETED FORM TO EMPLOYER. |
||||||
Call (808)
Auxiliary aids and services are available upon request. Please call (808)
Important Notice about Language Assistance: This document contains important information. If you need language assistance at no cost to you, please contact us by phone or in person immediately.
It is the policy of the Department of Labor and Industrial Relations that no person shall, on the basis of race, color, sex, marital status, religion, creed, ethnic origin, national origin, age, disability, ancestry, arrest/court record, sexual orientation, and National Guard participation, be subjected to discrimination, excluded from participation in, or denied the benefits of the Department’s services, programs, activities, or employment.
After you have gathered the necessary information, you can proceed to fill out the Hawaii HC-5 form. This form is essential for notifying your employer about your health care coverage status. Ensure that all information is accurate and complete before submission.
Filling out the Hawaii HC 5 form can be straightforward, but several common mistakes can lead to complications. One significant error is failing to identify the correct principal employer. Employees often overlook the requirement to select the employer who pays the most wages or works the most hours. This choice is crucial because it determines which employer is responsible for providing health care coverage. If this designation is incorrect, the employee may face gaps in coverage or confusion regarding their health care benefits.
Another common mistake is neglecting to check the appropriate boxes on the form. Employees might skip this step or misinterpret the options available. Each box corresponds to specific circumstances, such as claiming an exemption or waiving coverage. Not marking the correct option can lead to misunderstandings between the employee and employer, potentially resulting in a denial of health care coverage that the employee is entitled to receive.
Inaccurate personal information is yet another frequent error. Employees sometimes provide incorrect details, such as their address, phone number, or even their name. This information is essential for ensuring that the employer can contact the employee regarding health care matters. A simple typo can create significant delays and complications in processing the form, leading to unnecessary stress for the employee.
Lastly, many employees forget to keep a copy of the completed form for their records. It is critical to retain this documentation as proof of notification to the employer. Without a copy, employees may struggle to resolve disputes or clarify their health care status in the future. Keeping a signed copy ensures that employees have evidence of their submissions and can reference it if needed.
The Hawaii HC-5 form is a critical document for employees working for multiple employers or those seeking health care coverage exemptions. Alongside this form, several other documents may be necessary to ensure compliance with health care regulations in Hawaii. Here’s a list of commonly used forms that complement the HC-5.
Understanding these forms can help employees navigate their health care options effectively. Each document serves a specific purpose, contributing to a comprehensive approach to health care coverage in Hawaii.
N-15 - The agreement's duration is month-to-month, providing flexibility for termination by either party.
Food Permit Hawaii - In case of any issues, applicants can contact the Sanitation Branch via the provided phone number.
The Texas RV Bill of Sale form plays a crucial role in documenting the details of the transaction between the buyer and seller, ensuring a smooth transfer of ownership. It is recommended that both parties familiarize themselves with the process, and for convenience, the editable form can be accessed at https://billofsaleforvehicles.com/editable-texas-rv-bill-of-sale.
Hawaii T1 - The trade name being registered must be clearly stated on the form.
The Hawaii HC-5 form is a notification document used by employees to inform their employers about their health care coverage status. It is specifically designed for individuals who work for multiple employers, wish to claim an exemption from health care coverage, or need to change their employer designations. This form is essential for compliance with the Hawaii Prepaid Health Care Act.
This form should be used by employees who meet any of the following criteria:
The HC-5 form is not necessary for employees who:
Employees must provide specific information, including:
Employees can select from several options on the form, such as:
Employers are required to retain the completed and signed HC-5 form for a period of two years. This is crucial for record-keeping and compliance with state regulations.
After filling out the HC-5 form, employees should keep a copy for their records and submit the completed form to their employer. It is important to ensure that the employer receives this notification to maintain proper health care coverage.
For any questions or assistance related to the HC-5 form, employees can contact the Department of Labor and Industrial Relations at (808) 586-9188. Additional resources are available for those needing accommodations or auxiliary aids.
| Fact Name | Description |
|---|---|
| Purpose of Form | The HC-5 form is used by employees to notify their employers about health care coverage status, especially when working for multiple employers. |
| Governing Law | This form is governed by the Hawaii Prepaid Health Care Act, specifically under Chapter 393 of the Hawaii Revised Statutes. |
| Employee Instructions | Employees must keep a signed copy of the completed form for their records and provide the original to their employer. |
| Employer Responsibilities | Employers are required to maintain the completed form for two years and provide health care coverage as indicated by the employee's selections. |
Understanding the Hawaii HC 5 form is essential for employees navigating health care coverage in the state. However, several misconceptions often arise. Here are four common misunderstandings about this form:
Being informed about these misconceptions can help employees make better decisions regarding their health care coverage and ensure compliance with state regulations.