Free State Hawaii Tdi 45 Template
Free State Hawaii Tdi 45 Template
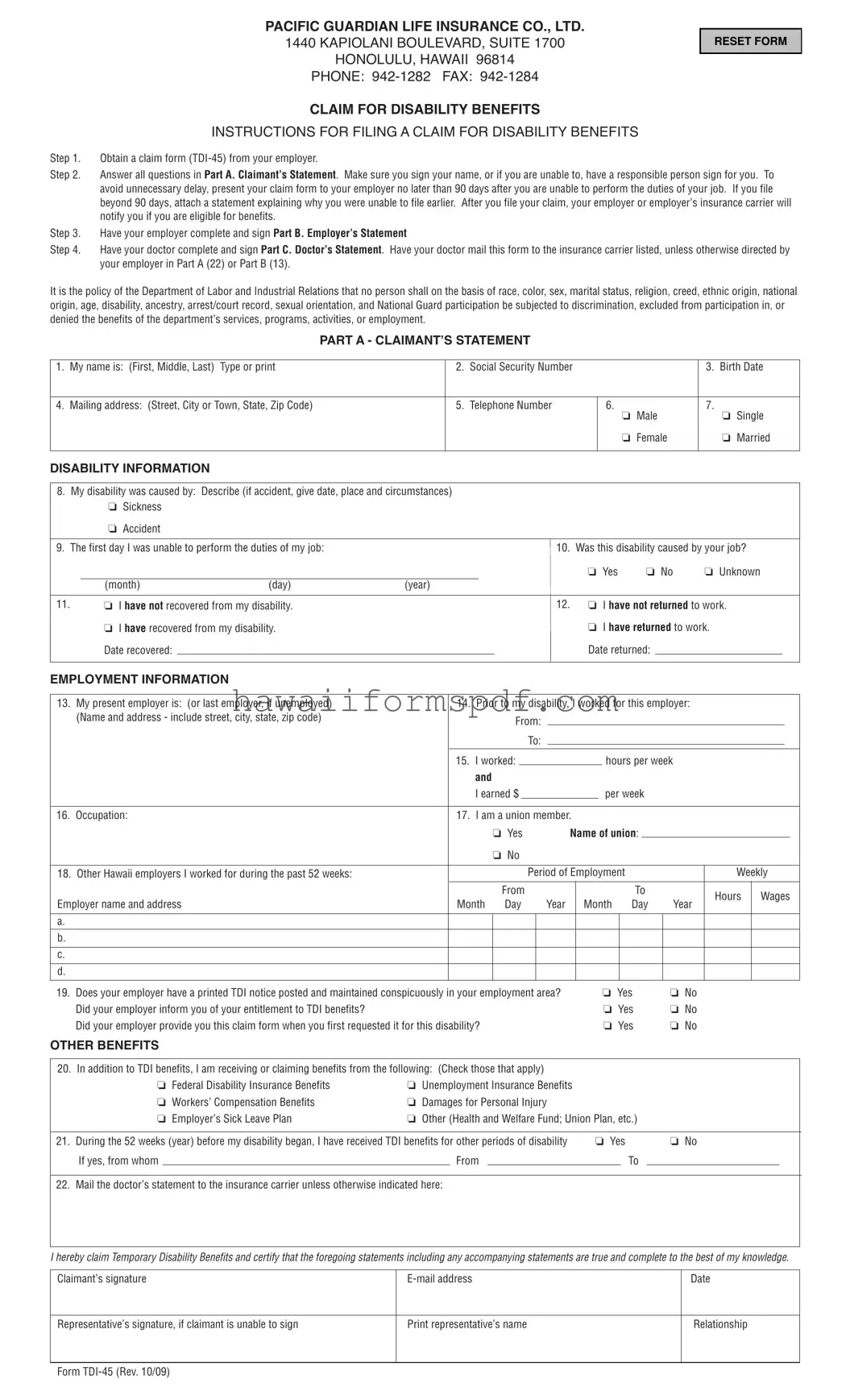
The State of Hawaii's TDI 45 form plays a crucial role in the process of applying for Temporary Disability Insurance (TDI) benefits. This form is specifically designed for individuals who are unable to work due to a disability, whether caused by an illness or an accident. To initiate a claim, claimants must first obtain the TDI 45 form from their employer and fill out Part A, which includes personal information and details about the disability. Timeliness is essential; claims should be submitted within 90 days of the onset of the disability to avoid delays. Employers are required to complete Part B, providing necessary information about the claimant's employment status and wages. Additionally, a doctor must fill out Part C to verify the medical aspects of the claim. Each section of the form is structured to gather specific information, ensuring that the claim is processed efficiently. Importantly, the TDI program is designed to be accessible and equitable, prohibiting discrimination based on various personal characteristics. Understanding the steps involved in completing the TDI 45 form is vital for anyone seeking disability benefits in Hawaii.
PACIFIC GUARDIAN LIFE INSURANCE CO., LTD.
1440 KAPIOLANI BOULEVARD, SUITE 1700
HONOLULU, HAWAII 96814
PHONE:
CLAIM FOR DISABILITY BENEFITS
INSTRUCTIONS FOR FILING A CLAIM FOR DISABILITY BENEFITS
RESET FORM
Step 1. Obtain a claim form
Step 2. Answer all questions in Part A. Claimant’s Statement. Make sure you sign your name, or if you are unable to, have a responsible person sign for you. To avoid unnecessary delay, present your claim form to your employer no later than 90 days after you are unable to perform the duties of your job. If you file beyond 90 days, attach a statement explaining why you were unable to file earlier. After you file your claim, your employer or employer’s insurance carrier will notify you if you are eligible for benefits.
Step 3. Have your employer complete and sign Part B. Employer’s Statement
Step 4. Have your doctor complete and sign Part C. Doctor’s Statement. Have your doctor mail this form to the insurance carrier listed, unless otherwise directed by your employer in Part A (22) or Part B (13).
It is the policy of the Department of Labor and Industrial Relations that no person shall on the basis of race, color, sex, marital status, religion, creed, ethnic origin, national origin, age, disability, ancestry, arrest/court record, sexual orientation, and National Guard participation be subjected to discrimination, excluded from participation in, or denied the benefits of the department’s services, programs, activities, or employment.
PART A - CLAIMANT’S STATEMENT
1. |
My name is: (First, Middle, Last) Type or print |
2. |
Social Security Number |
|
3. |
Birth Date |
|
|
|
|
|
|
|
4. |
Mailing address: (Street, City or Town, State, Zip Code) |
5. |
Telephone Number |
6. |
7. |
|
|
|
|
|
o Male |
|
o Single |
|
|
|
|
o Female |
|
o Married |
|
|
|
|
|
|
|
DISABILITY INFORMATION
8.My disability was caused by: Describe (if accident, give date, place and circumstances) o Sickness
oAccident
9. |
The first day I was unable to perform the duties of my job: |
10. |
Was this disability caused by your job? |
||||||||
|
|
|
|
|
|
|
o Yes |
o No |
o Unknown |
||
|
|
(month) |
(day) |
(year) |
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|||
11. |
|
o I have not recovered from my disability. |
12. |
o I have not returned to work. |
|||||||
|
|
o I have recovered from my disability. |
|
|
|
o I have returned to work. |
|||||
|
|
Date recovered: |
|
|
|
|
Date returned: |
|
|
|
|
EMPLOYMENT INFORMATION
13. |
My present employer is: (or last employer, if unemployed) |
|
14. |
Prior to my disability, I worked for this employer: |
|
|
|
|
||||||||||||||||||
|
(Name and address - include street, city, state, zip code) |
|
|
|
|
|
From: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
To: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
15. |
I worked: |
|
|
|
|
|
|
|
hours per week |
|
|
|
|
|||||||||
|
|
|
|
|
|
and |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I earned $ |
|
|
|
|
|
per week |
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
16. |
Occupation: |
|
17. |
I am a union member. |
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
o Yes |
|
Name of union: |
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
o No |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
18. |
Other Hawaii employers I worked for during the past 52 weeks: |
|
|
|
|
|
|
|
Period of Employment |
|
|
|
|
Weekly |
||||||||||||
|
|
|
|
|
|
|
|
From |
|
|
|
|
|
|
To |
|
Hours |
Wages |
||||||||
Employer name and address |
|
|
Month |
Day |
Year |
|
Month |
Day |
Year |
|||||||||||||||||
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
a. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
b. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
c. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
d. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
19. |
Does your employer have a printed TDI notice posted and maintained conspicuously in your employment area? |
|
|
|
o Yes |
o No |
|
|
|
|
||||||||||||||||
|
Did your employer inform you of your entitlement to TDI benefits? |
|
|
|
|
|
|
|
|
|
|
|
|
|
o Yes |
o No |
|
|
|
|
||||||
|
Did your employer provide you this claim form when you first requested it for this disability? |
|
|
|
|
|
|
|
|
o Yes |
o No |
|
|
|
|
|||||||||||
OTHER BENEFITS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
20. In addition to TDI benefits, I am receiving or claiming benefits from the following: (Check those that apply) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
o Federal Disability Insurance Benefits |
o Unemployment Insurance Benefits |
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
o Workers’ Compensation Benefits |
o Damages for Personal Injury |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
o Employer’s Sick Leave Plan |
o Other (Health and Welfare Fund; Union Plan, etc.) |
|
|
|
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
21. |
During the 52 weeks (year) before my disability began, I have received TDI benefits for other periods of disability |
|
o Yes |
|
|
|
o No |
|
|
|
|
|||||||||||||||
|
If yes, from whom |
|
|
|
From |
|
|
|
|
|
|
|
|
|
|
|
To |
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
22. Mail the doctor’s statement to the insurance carrier unless otherwise indicated here: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I hereby claim Temporary Disability Benefits and certify that the foregoing statements including any accompanying statements are true and complete to the best of my knowledge.
Claimant’s signature |
Date |
|
|
|
|
Representative’s signature, if claimant is unable to sign |
Print representative’s name |
Relationship |
|
|
|
Form
_____% PREMIUM PAID BY EMPLOYER
PART B - EMPLOYER’S STATEMENT
IMPORTANT: To enable your disabled employee to receive TDI benefits within 10 days as required by law, it is imperative that you complete the following information for prompt submittal to your insurance carrier.
1. |
Claimant’s Name |
|
|
|
2. |
Claimant’s Occupation |
|
|
|
|
|
|
|
|
3. Employer Department of Labor No. |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||
4. Group and Account Number |
|
|
5. Firm or Trade Name |
|
|
|
|
|
6. Business Address |
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
7. |
In reporting wage information below, use gross wages, which include wages and all other |
8. |
Worked: |
|
|
o |
|
|
o |
|||||||||||||||||||||||
|
remuneration such as commissions, bonuses, tips and the cash value of meals, lodging, etc. |
|
|
|
Date hired: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
Answer either A, B, or C. |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(month) |
|
(day) |
(year) |
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Date last worked prior to disability: |
|
|
|
|
|
|
|
||||||||
|
A. If claimant was paid on a salary basis, enter claimant’s weekly or monthly salary earned |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
in the last week or month prior to the date claimant’s disability began: |
|
|
|
|
|
|
|
|
|
|
(month) |
|
(day) |
(year) |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If returned to work, give date: |
|
|
|
|
|
|
|
|
|
||||||
|
Week $ ______________ |
Month $ ______________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
(month) |
|
(day) |
(year) |
|||||||
|
B. If paid on an hourly basis, give rate per hour $ _____________. Enter the weekly |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||
|
9. Check days normally worked: |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
earnings for the past 8 weeks prior to the date disability began, including the last |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
o Sun o |
|
Mon |
o Tues o Wed o |
Thurs o Fri o Sat |
|||||||||||||||||||||||||
|
date worked. (Include reported tips) |
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
If on rotation, give the number of days worked per week |
|
|
|
|
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
Weekending |
|
|
|
|
|
|
|
10. |
Enter the following for the last 52 weeks prior to the date the |
||||||||||||||||||||
Week |
|
|
|
|
|
No. Days |
|
Gross |
||||||||||||||||||||||||
No. |
Month |
|
Day |
Year |
|
Worked |
|
Amount |
|
|
employee’s disability began: |
|
|
|
|
|
|
|
|
|
||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
1 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Calendar |
|
|
No. of |
|
No. of Hours |
|
Total Wages |
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
Quarter Ending |
|
Weeks Worked |
|
Worked Per Wk. |
|
Earned |
|||||||||||||
|
2 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
4 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
5 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
7 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
8 |
|
|
|
|
|
|
|
|
|
|
|
|
11. |
Do you think this disability was caused by the claimant’s job? |
|||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
o Yes |
o No |
o Unknown |
|
|
|
|
|
|
|
|||||||
Total |
XXXX |
|
XXXX |
XXXX |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Was an Employer’s Report of Industrial Injury |
||||||||||||||||
|
C. If claimant received any or all earnings on a commission or piecework basis, enter these |
|
|
|||||||||||||||||||||||||||||
|
|
|
o Yes |
o No |
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
earnings for the last 52 weeks prior to the date claimant’s disability began: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
This covers the period: |
|
|
|
|
|
|
|
|
|
|
|
If yes, advise name and address of Worker’s Compensation Carrier |
|||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||
|
From: ______________ through ______________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
|
|
(month/day/year) |
(month/day/year) |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
Earnings: $ ______________ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
13. |
Mail the doctor’s statement to: |
|
|
|
|
|
|
|
12. |
Has or will this employee receive all or any portion of the |
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
period of disability covered by this claim? |
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Wages? |
o Yes |
o No |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Salary? |
o Yes |
o No |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Sick leave pay? |
o Yes |
o No |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Vacation pay? |
o Yes |
o No |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Separation pay? |
o Yes |
o No |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
If yes, show period: |
|
|
|
|
|
|
Amount |
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
From: |
|
|
|
|
|
|
|
(mo/day/yr) |
|
$_________ |
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Through: |
|
|
|
|
|
|
(mo/day/yr) |
|
|
|||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
I hereby certify that the above information is true and complete to the best of my knowledge.
Signature of employer or employer’s representative
Title
Date
Telephone No. |
Fax No. |
PART C - DOCTOR’S STATEMENT
IMPORTANT: Please complete and mail within 7 working days after examination to the insurance carrier listed above unless otherwise directed in Part A (22) or Part B (13).
1. |
Claimant’s Name |
|
|
|
|
|
2. Age |
3. |
Sex |
|||
|
|
|
|
|
|
|
|
|
||||
4. |
Physical requirements of claimant’s occupation as related by claimant: |
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
5. |
Diagnosis: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
6. |
If pregnancy, advise expected date of birth __________________________________. If disability is pregnancy with complications, advise complications above. |
|||||||||||
|
||||||||||||
|
|
|
|
|
|
|
|
|
||||
7. |
Was claimant’s disability caused by claimant’s employment? |
o Yes |
o No |
|
|
|
||||||
|
If yes, was Physician’s Report |
If yes, filed with _____________________________________________________________ |
||||||||||
|
|
|
|
|
|
|
|
|
|
|||
8. |
Was claimant hospitalized? |
o Yes |
o No |
If yes, from ______________________ to ______________________ |
|
|
|
|||||
|
Surgery indicated? |
o Yes |
o No |
Type _____________________________________________________________ |
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
9. |
Complete the following: |
|
|
|
|
|
|
Month |
|
Day |
|
Year |
|
|
|
|
|
|
|
|
|
|
|
||
|
Date of your first treatment of this disability |
|
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
||||||
|
First date claimant unable to perform the duties of employment (see #4 above) |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|||
|
Date of your most recent treatment of this disability |
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
|
|
||||||
|
Date claimant will be able to perform usual work (estimate) (DO NOT use “undetermined” or “unknown”) (See #4 above) |
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|||||
10. |
Are you referring claimant to another physician? |
o Yes |
o No |
If yes, give name ____________________________________________________ |
||||||||
|
OR |
|
|
|
|
|
|
|
|
|
|
|
|
Was claimant referred to you? |
|
|
o Yes |
o No |
If yes, give name ____________________________________________________ |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
I hereby certify that the above information is true and complete to the best of my knowledge.
Doctor’s name (Please print)
Office Address
Doctor’s signature
Date
Telephone No.
Fax No.
Filling out the State Hawaii TDI 45 form involves several important steps. This form is necessary for claiming disability benefits. It requires information from the claimant, employer, and doctor. Be sure to complete each part accurately to ensure a smooth process.
Once the form is submitted, your employer or their insurance carrier will review your claim and notify you of your eligibility for benefits. Make sure to keep copies of all documents for your records.
Filling out the State Hawaii TDI 45 form can be a straightforward process, but many people make common mistakes that can delay their claims. One of the most frequent errors is failing to complete all sections of Part A, the Claimant’s Statement. Each question must be answered thoroughly. Leaving even one question blank can lead to unnecessary delays in processing your claim.
Another mistake is not signing the form. Claimants often forget to sign their name, or they may ask someone else to sign without ensuring that person is authorized. If you cannot sign, make sure a responsible person signs on your behalf and includes their relationship to you. This oversight can cause your claim to be rejected.
Many individuals also miss the 90-day filing deadline. It’s crucial to submit your claim within this timeframe. If you file late, you must include a statement explaining why. Not doing so can result in your claim being denied. Keep track of your dates and submit your claim as soon as possible.
People sometimes fail to provide detailed information about their disability. In question 8, it’s important to describe how the disability occurred, including the date, place, and circumstances if it was an accident. Vague responses can lead to confusion and may require additional follow-up from the insurance carrier.
Another common issue arises in Part B, the Employer’s Statement. Employers must complete and sign this section promptly. Delays from the employer’s side can slow down the entire process. Employers should ensure that they provide accurate wage information and that all required fields are filled out.
Claimants often overlook the requirement to report other benefits they are receiving. In question 20, it’s essential to disclose any additional benefits, such as unemployment or workers’ compensation. Failing to do this can raise red flags and complicate the claim process.
Lastly, many people forget to check the mailing instructions for the doctor’s statement in Part C. The form requires that this statement be mailed to the correct insurance carrier. If the doctor sends it to the wrong address, it could delay your claim significantly. Always double-check that the form is sent to the right place.
The State of Hawaii TDI-45 form is a crucial document for individuals seeking temporary disability benefits. However, several other forms and documents often accompany this claim to ensure a comprehensive evaluation of eligibility and benefits. Below is a list of these related documents, each serving a specific purpose in the claims process.
Understanding these accompanying forms and documents is essential for individuals navigating the disability benefits process in Hawaii. Each document plays a vital role in ensuring that claims are processed accurately and efficiently, ultimately supporting claimants during their time of need.
Hawaii Real Estate Purchase Contract - The agreement covers proration of current year taxes and other fees through the closing date.
A Wyoming Promissory Note is a legal document that outlines a borrower's promise to repay a specific amount of money to a lender under agreed-upon terms. This form serves as a crucial tool for both parties, ensuring clarity and protection in financial transactions. For more information and resources, you can visit https://promissorynotepdf.com/ to help you get started on your own Promissory Note.
Hawaii Form N-15 - Seek assistance if you encounter confusion regarding your filing status or deductions.
Hawaii State Tax Forms - For any fuel used off public highways, it's critical to have this certificate ready at purchase.
The TDI-45 form, also known as the Claim for Disability Benefits, is a document used in Hawaii for individuals seeking temporary disability insurance benefits. This form allows claimants to report their disability status and provides necessary information for their employer and healthcare provider to complete their claims.
Filling out the TDI-45 form involves several steps:
Make sure to submit the form within 90 days of your disability to avoid delays.
In Part A, you will need to provide personal details, including:
Accurate and complete information helps expedite the claims process.
If you are unable to file your claim within the 90-day timeframe, you must attach a statement explaining the reason for the delay. This is crucial for ensuring that your claim is still considered for benefits.
Yes, you can receive other benefits while claiming TDI. The TDI-45 form allows you to indicate if you are receiving or claiming additional benefits such as federal disability insurance, unemployment insurance, or workers’ compensation. Be sure to check all applicable boxes on the form.
The claimant's doctor is responsible for completing and submitting the Doctor’s Statement (Part C) to the insurance carrier. This step is essential as it provides medical verification of your disability.
After submitting the TDI-45 form, your employer or their insurance carrier will review your claim and notify you of your eligibility for benefits. This process typically occurs within ten days, so keep an eye on your mail or email for updates.
| Fact Name | Description |
|---|---|
| Form Title | The form is officially titled "Claim for Disability Benefits" and is designated as TDI-45. |
| Governing Law | This form is governed by Hawaii's Temporary Disability Insurance (TDI) law, specifically HRS Chapter 392. |
| Filing Deadline | Claims must be submitted within 90 days of the inability to perform job duties to avoid delays. |
| Claimant's Statement | Part A requires the claimant to provide personal information, including their name, social security number, and details about their disability. |
| Employer's Statement | Part B must be completed by the employer, providing necessary employment details to support the claim. |
| Doctor's Statement | Part C requires the claimant's doctor to complete and certify the medical information related to the disability. |
| Non-Discrimination Policy | The form includes a statement ensuring that no person shall face discrimination in accessing TDI benefits. |
| Additional Benefits | Claimants must disclose any other benefits they are receiving, such as unemployment or workers’ compensation. |
| Signature Requirement | The claimant must sign the form, or a representative may sign if the claimant is unable to do so. |
| Submission Instructions | The completed form should be submitted to the insurance carrier indicated on the form, following the specified steps. |
Misconception 1: The TDI 45 form is only for employees who have been injured at work.
This is not accurate. The TDI 45 form can be used for any disability, whether caused by an accident or illness, regardless of its relation to the workplace. Claimants must simply provide the appropriate details about their condition.
Misconception 2: You must submit the TDI 45 form immediately after becoming disabled.
While timely submission is important, claimants have up to 90 days to file the form. If filing occurs after this period, it is necessary to include a statement explaining the delay. This allows for some flexibility in the process.
Misconception 3: Only full-time employees are eligible for TDI benefits.
This is incorrect. Both full-time and part-time employees can qualify for TDI benefits as long as they meet the necessary criteria and have contributed to the program. Employment status does not exclude part-time workers from receiving assistance.
Misconception 4: Employers have no responsibility in the TDI claim process.
Employers play a crucial role in the TDI claim process. They are required to complete and sign the Employer's Statement section of the TDI 45 form. Their timely cooperation can significantly affect the speed at which benefits are processed.
When filling out and using the State Hawaii TDI 45 form, keep these key takeaways in mind: